Reproduction and Development for the DAT
/Learn key DAT concepts related to fertilization, cleavage, gastrulation, neurulation, and organogenesis, plus practice questions and answers

Learn everything you need to know about reproduction and development for the dat
Table of Contents
Part 1: Introduction to reproduction and development
Part 2: Reproductive overview
a) Endocrine control
b) Spermatogenesis
c) Oogenesis
Part 3: Fertilization and early development
a) Fertilization
b) Cleavage, blastulation, and implantation
c) Gastrulation
Part 4: Germ cell layers
a) Endoderm
b) Mesoderm
c) Ectoderm
Part 5: Neurulation
Part 6: Later development
a) Stages of pregnancy
b) Cell specialization
c) Apoptosis and regeneration
Part 7: High-yield terms
Part 8: Questions and answers
----
Part 1: Introduction to the reproductive system
As you delve into the intricacies of human anatomy, physiology, and biochemistry, the remarkable speed of human reproduction may appear almost magical. Within merely eight weeks following fertilization, a solitary zygote transforms rapidly into a multicellular embryo, initiating the formation of various organ systems.
This guide aims to offer a concise overview of reproductive endocrinology and cellular physiology. Subsequently, we'll explore the pivotal developmental stages, starting from fertilization and progressing through blastulation, gastrulation, and neurulation. Lastly, this guide will enable you to test your knowledge with DAT-style practice problems.
----
Part 2: Reproductive overview
a) Endocrine control
The HPG axis, comprising the hypothalamus, anterior pituitary, and gonads, orchestrates reproductive functions. Triggered by the hypothalamus, gonadotropin-releasing hormone (GnRH) influences the anterior pituitary. This, in turn, prompts the secretion of follicle-stimulating hormone (FSH) and luteinizing hormone (LH).
FSH and LH exert direct effects on gonads, displaying distinct roles in male and female physiology. In females, FSH nurtures the growth and maturation of follicles within the ovaries. Follicles are immature cells that play a crucial role in egg development. Conversely, in males, FSH stimulates spermatogenesis—the generation of sperm.
LH orchestrates ovulation and spurs estrogen synthesis in females. Estrogen not only thickens the uterine lining but also influences secondary sexual characteristics. Additionally, LH triggers progesterone synthesis during the menstrual cycle (pictured below), influencing the follicular phase, ovulation, and the luteal phase.

FIGURE 1: MENSTRUAL CYCLE RELATIVE CHANGES IN ENDOCRINE HORMONES
For males, LH drives testosterone production. Testosterone is pivotal in developing secondary sexual traits during puberty and fostering sexual drive. It also plays a pivotal role in the male fetus, directing the development of male genitalia.
Although their chromosomal sex is determined, early embryos initially lack sexual differentiation. Testosterone plays a vital role in inducing early genitalia to follow a male developmental course.

FIGURE 2: HPG AXIS FOR FEMALES

FIGURE 3: HPG AXIS FOR MALES
In normal physiology, male and female germ cells mature into distinct structures—testes storing sperm (male germ cells) and ovaries housing eggs (female germ cells). Specialized helper cells, such as Sertoli cells and Leydig cells for sperm development and granulosa cells plus theca cells for oocyte formation, support their growth. The process of producing sperm and egg cells, termed gametogenesis, results in the generation of gametes.
b) Spermatogenesis
The male reproductive system comprises both internal and external structures, with the testes serving as the male gonads.
Spermatogenesis is the process of sperm formation and occurs in the seminiferous tubules of the testes. It begins with a diploid spermatogonium undergoing mitosis, transforming into a diploid primary spermatocyte. Subsequent meiosis I results in two haploid secondary spermatocytes. Each of these then undergoes meiosis II, producing four haploid spermatids. These spermatids further mature into spermatozoa.
This intricate meiotic division and maturation take place within the testicular seminiferous tubules. Sertoli cells assist in spermatogenesis and are stimulated by FSH. Leydig cells also participate in spermatogenesis and are activated by LH to produce testosterone.

FIGURE 4: SPERMATOGENESIS
Sperm gain motility and reside in the epididymis, where they await ejaculation. Post-maturation, each spermatid becomes a haploid spermatozoon. During ejaculation, sperm traverse the vas deferens, the ejaculatory duct, and finally the urethra, facilitating their exit from the penis.

FIGURE 5: SPERM CELL STRUCTURE
A head of a sperm cell contains elements crucial to the reproductive process. The acrosome, derived from the Golgi apparatus, acts as a cap that enables the sperm to penetrate the oocyte during fertilization. The nucleus within the head houses the DNA. The midpiece of the sperm contains numerous mitochondria that provide the energy necessary for the flagellum, or tail, to facilitate movement. This evolved energy production capacity aids the sperm in its primary function of traveling through the female reproductive tract to fertilize an oocyte.
c) Oogenesis
The female reproductive system comprises internal structures, predominantly the ovaries acting as the female gonads. Besides producing estrogen and progesterone, the ovaries contain ova (eggs).
Oogenesis involves the formation of oocytes in females. Unlike spermatogenesis that commences around puberty in males, oogenesis begins prenatally.
During prenatal development, diploid oogonia—ovarian stem cells—undergo mitosis, giving rise to diploid primary oocytes. These primary oocytes wait at prophase I until puberty. Hence, at birth, all existing oogonia are arrested as primary oocytes in prophase I.
Upon reaching puberty, meiotic division resumes for these oocytes. In each menstrual cycle, one primary oocyte enclosed within a follicle completes meiosis I. This process forms a haploid secondary oocyte and a smaller polar body that is discarded due to minimal cytoplasm.
The secondary oocyte halts at metaphase II. During ovulation, the follicle ruptures, releasing the developing oocyte into the Fallopian tubes.
Crucially, meiosis II concludes only upon binding of a sperm cell to the oocyte. Upon binding, the oocyte finishes meiosis II, dividing into a larger ovum ready for fertilization and a smaller, secondary polar body.
Granulosa cells are activated by FSH to create a protective outer covering for the oocyte known as the zona pellucida. Theca cells, also within the ovaries and stimulated by LH, produce androstenedione, an estrogen precursor.
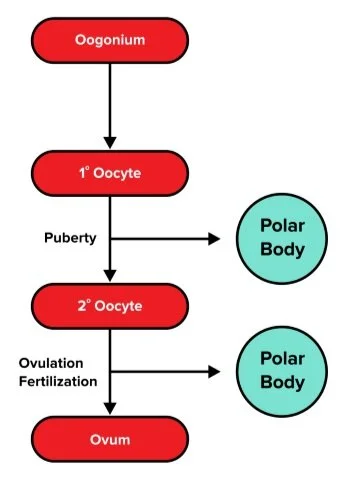
FIGURE 6: OOGENESIS
Every month, an ovum is released into the abdominal cavity and travels through a fallopian tube that links the ovaries to the uterus. Post-intercourse, when a sperm cell enters the cervix, it journeys to the fallopian tube for potential fertilization with the egg.
----
Part 3: Fertilization and early development
a) Fertilization
Fertilization marks the fusion of a sperm cell and an ovum. It typically occurs in the widest section of the Fallopian tube known as the ampulla. Here, the sperm encounters the secondary oocyte. How does this interaction complete the oocyte's meiotic division?
An acrosomal reaction unfolds as the sperm releases enzymes from its head's cap, aiding its penetration of the zona pellucida. Upon breaking through the cell membrane, the sperm delivers its nucleus into the oocyte, culminating in the completion of meiosis II. The once-secondary oocyte is now an ovum.
Subsequently, a cortical reaction takes place, raising calcium levels. Although beyond the DAT scope, this reaction prevents polyspermy, where multiple sperm fertilize one egg. In humans, polyspermy typically results in nonviable conditions, as fertilization by two sperm leads to a fused cell with a 3N ploidy, hindering mitotic division and development.
Following fertilization, a single diploid cell termed the zygote emerges, harboring its distinct genetic material. Remember, genetic sex hinges on the 23rd pair of chromosomes: an XX karyotype denotes female development, while an XY karyotype signals male development.
b) Cleavage, blastulation, and implantation
As the zygote embarks on its journey towards the endometrium for implantation, it undergoes a flurry of cell divisions known as cleavage. This rapid division, unlike standard mitotic processes, duplicates genetic material without substantial cell growth. This progression shapes the emerging multicellular organism, now known as an embryo. The embryo continues dividing until it forms a 16-cell structure called a morula. The morula resembles a solid sphere of densely packed cells and is indistinguishable between its interior and exterior.
The morula undergoes a profound transformation, transitioning into a blastocyst through a process called blastulation. In contrast to the uniform structure of the morula, the blastocyst comprises three primary components. First, it features a central hollow cavity filled with fluid known as the blastocoel. Second, the inner cell mass (ICM), an inner layer of cells within the blastocyst, holds the potential to develop into the fetus. Lastly, the blastocyst's exterior is formed by trophoblast cells.
Cells housed within the inner cell mass are set to evolve into various body structures. At this stage, these stem cells exhibit pluripotency. This differs from the earlier totipotent cells found in the morula, capable of forming both the body and the extraembryonic membranes. While totipotent cells can become any cell type, pluripotent stem cells are limited to developing into body cells.
During blastulation, the developing embryo travels through the Fallopian tube towards the uterus. Upon reaching the uterus, trophoblast cells breach the endometrium, initiating the formation of the placenta. This fully operational endocrine organ evolves during pregnancy and is expelled after childbirth. The placenta also fosters gas, nutrient, and antibody exchange without mixing blood. While the intricacies of placental development extend beyond the DAT scope, acknowledging its role as a maternal and fetal organ for essential exchanges is crucial.

Gain instant access to the most digestible and comprehensive DAT content resources available. Subscribe today to lock in the current investments, which will be increasing in the future for new subscribers.